Anatomy & Education
The lacrimal system produces, distributes, and drains tears. A healthy tear film is essential for corneal health, clear vision, and comfort. When any part of the drainage pathway is obstructed, tears overflow onto the cheek (epiphora) and may become a source of chronic infection.
The lacrimal system has two functional components: the secretory system (which produces tears) and the excretory system (which drains them). The two components must be in balance — inadequate drainage causes overflow, while inadequate production causes dry eye.
Tears flow across the ocular surface from lateral to medial with each blink, collecting in the medial lake (lacus lacrimalis) near the inner corner of the eye. They then enter the drainage system through small openings at the inner edge of each lid margin.
The tear film is a three-layer structure essential for optical clarity and corneal nutrition:
Lipid Layer (outer)
Source: Meibomian glands (in tarsal plate)
Prevents evaporation; stabilizes the tear film
Aqueous Layer (middle)
Source: Lacrimal gland & accessory glands (Krause, Wolfring)
Provides oxygen, nutrients, and antibacterial proteins to the cornea
Mucin Layer (inner)
Source: Goblet cells (conjunctiva)
Anchors the tear film to the hydrophobic corneal epithelium
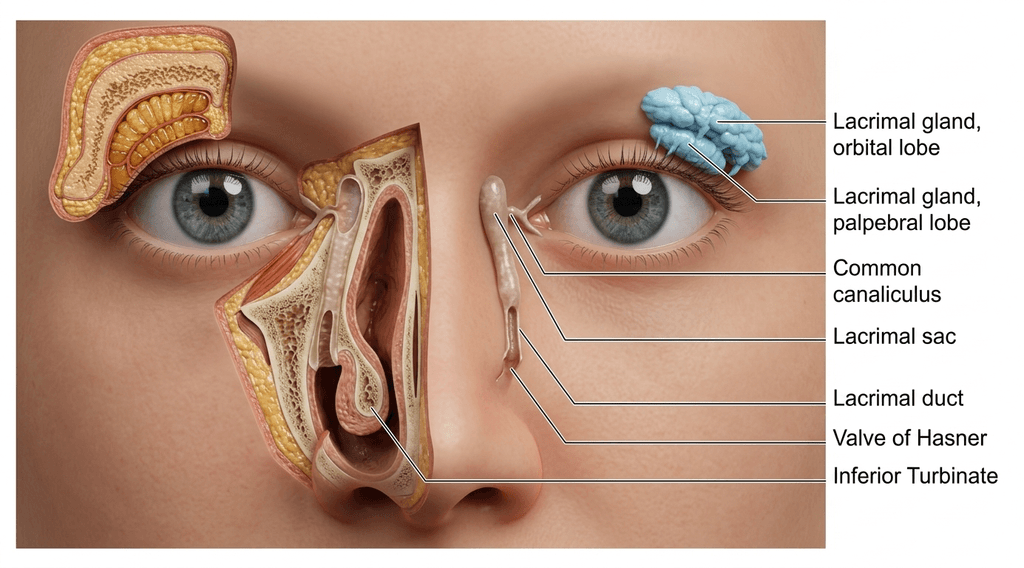
Lacrimal gland location: The main lacrimal gland sits in the superolateral orbit in the lacrimal fossa of the frontal bone. It is divided into orbital and palpebral lobes by the lateral horn of the levator aponeurosis. During upper eyelid blepharoplasty, the lacrimal gland is occasionally prolapsed and can be mistaken for orbital fat — careful identification is essential.
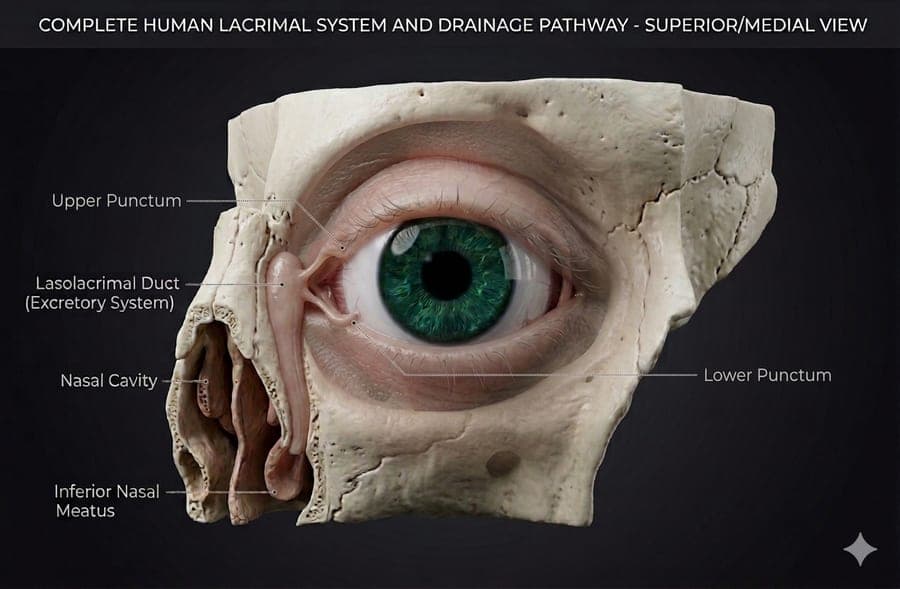
Tears drain through a series of structures from the ocular surface into the nasal cavity:
Two small oval openings — one on the upper lid and one on the lower lid — located at the medial end of each lid margin on a small elevation called the lacrimal papilla. Each is approximately 0.3 mm in diameter. Punctal stenosis (narrowing) is a common cause of tearing.
Narrow tubular channels leading from each punctum to the lacrimal sac. Each canaliculus has a short vertical portion (2 mm) then turns medially for a horizontal portion (8–10 mm). The upper and lower canaliculi typically join into a common canaliculus (90% of people) before entering the lacrimal sac.
A mucosal fold at the junction of the common canaliculus and lacrimal sac that acts as a one-way valve, preventing reflux of tears back from the sac into the canaliculi.
A small reservoir (12–15 mm tall, 4–8 mm wide) lying in the lacrimal fossa — a groove in the medial orbital wall formed by the lacrimal bone and frontal process of the maxilla. The sac sits anterior to the orbital septum, between the anterior and posterior limbs of the medial canthal tendon.
A bony canal approximately 12–18 mm long running inferolaterally within the maxillary bone to open into the inferior nasal meatus. Its lower end is guarded by the valve of Hasner — a mucosal fold that prevents nasal air from blowing back up the duct. This valve fails to open in congenital NLDO.
Clinical importance: Any laceration medial to the punctum carries a high risk of canalicular involvement. Canalicular lacerations must be repaired within 24–48 hours with a silicone stent to maintain luminal patency during healing.
The lacrimal sac lies in the lacrimal fossa at the medial orbital wall. It is the target structure in dacryocystorhinostomy (DCR) surgery, in which a new bony window is created between the sac and the nasal cavity.
The nasolacrimal duct (NLD) runs inferiorly within the bony nasolacrimal canal, angled slightly laterally and posteriorly. It is entirely enclosed in bone for most of its length before opening into the inferior meatus of the nasal cavity.
Tear drainage is not passive — it depends on an active pumping mechanism powered by the orbicularis oculi muscle with each blink.
Orbicularis contraction (Horner's muscle) shortens and compresses the canaliculi, creating positive pressure that propels tears into the lacrimal sac.
Relaxation of orbicularis creates negative pressure in the canaliculi, drawing tears from the puncta into the canaliculi.
Between blinks, gravity and the ciliated epithelium lining the NLD help propel tears distally toward the nasal cavity.
Punctal stenosis
Site: Punctum
Punctal dilation or 3-snip punctoplasty →
Canalicular obstruction
Site: Canaliculus
Silicone intubation / Jones tube (CDCR) →
Dacryocystitis
Site: Lacrimal sac
Antibiotics + DCR surgery →
Congenital NLDO
Site: Valve of Hasner
Probing, intubation, or DCR →
Acquired NLDO (PANDO)
Site: NLD isthmus
Endoscopic or external DCR →
Functional epiphora
Site: Lacrimal pump
Eyelid tightening / ectropion repair →
Canalicular laceration
Site: Lower canaliculus
Stent + microsurgical repair within 48 hrs →
Contact us to discuss your concerns and learn about treatment options.
The distal valve of the nasolacrimal duct at its opening into the inferior nasal meatus. Failure of this valve to fully canalize before birth is the cause of congenital nasolacrimal duct obstruction (CNLDO) — affecting approximately 6% of newborns.
Dacryoadenitis
Site: Lacrimal gland
Antibiotics, biopsy if chronic →