Eyelid
Infections
Medical and surgical management of eyelid and orbital infections — preseptal and orbital cellulitis, dacryocystitis, herpes zoster, and more.
Medically reviewed by Andrew M. Goldbaum, MDOculoplastic SurgeonLast updated June 2026
Eyelid
Medical and surgical management of eyelid and orbital infections — preseptal and orbital cellulitis, dacryocystitis, herpes zoster, and more.
Medically reviewed by Andrew M. Goldbaum, MDOculoplastic SurgeonLast updated June 2026

Blepharitis is a chronic inflammation of the eyelid margins. It is one of the most common eyelid conditions and tends to recur despite treatment.
Blepharitis is usually inflammatory rather than infectious — chronic inflammation of the lid margins and meibomian glands (often with rosacea or Demodex), not a true infection. See the dedicated Blepharitis page for full detail.
Daily lid hygiene is the cornerstone of management: warm compresses applied for five minutes soften meibomian-gland secretions, followed by gentle lid-margin scrubbing with commercial lid-scrub wipes (now preferred over dilute baby shampoo, which can irritate the ocular surface). For moderate-to-severe disease, a course of oral doxycycline (50–100 mg daily for 6–12 weeks) is effective because of its anti-inflammatory effect on the meibomian glands, independent of its antibiotic properties.
Allergic conjunctivitis is the most common allergic eye condition, affecting approximately 20% of the U.S. population. It results from IgE-mediated histamine release when the conjunctiva is exposed to an allergen.
First-line treatment is allergen avoidance combined with topical antihistamine/mast-cell stabilizer drops such as olopatadine (Pataday), which are effective and well tolerated. Systemic antihistamines and, in more severe cases, brief topical corticosteroid courses may be required under ophthalmic supervision.
The orbital septum — a fibrous sheet running from the orbital rim to the tarsal plates — is the critical anatomic divider that determines the severity and management of periorbital infections.
Infection confined to the eyelid and soft tissue anterior to the orbital septum. The globe and orbit are not involved: extraocular movements, pupil reactions, and visual acuity are normal.

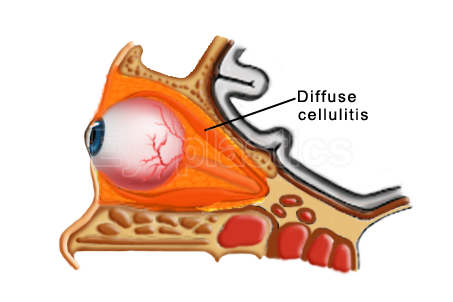
Infection posterior to the orbital septum, involving the orbital fat and structures. Ninety percent of cases arise from direct extension of bacterial sinusitis. This is an ophthalmic emergency.
Orbital cellulitis is a vision- and life-threatening emergency. Any patient with proptosis, restricted eye movement, or decreased vision requires urgent CT imaging and IV antibiotic therapy.


Herpes zoster ophthalmicus (HZO) occurs when the varicella-zoster virus — dormant in the trigeminal ganglion after childhood chickenpox — reactivates and travels along the first division of the trigeminal nerve (V1), affecting the forehead, scalp, upper eyelid, and eye.
Read the full guide to shingles in the eye (herpes zoster ophthalmicus) → — including how the herpesvirus family differs and where it strikes (skin, cornea, or orbit).
Oral antiviral therapy (acyclovir, valacyclovir, or famciclovir) should be started within 72 hours of rash onset to reduce severity, duration, and the risk of postherpetic neuralgia. Oculoplastic intervention may be required later to correct eyelid scarring, ectropion, or ptosis that results from cicatricial changes.
Prevention: The Shingrix vaccine (two doses) is recommended for all adults aged 50 and older, regardless of prior shingles history. It reduces the overall risk of shingles by roughly 90% and substantially lowers the risk of postherpetic neuralgia.
Infections of the tear-drainage system — the lacrimal sac and canaliculi — are a distinct group of periorbital infections that often require surgical management for definitive cure.
Dacryocystitis is infection of the lacrimal sac, caused by stasis of tears behind a blocked nasolacrimal duct. It presents as a painful, red, swollen mass at the inner corner of the lower eyelid.
Canaliculitis is infection of the small tear-drainage channels (canaliculi) connecting the puncta to the lacrimal sac. It presents with redness, swelling, and yellow discharge at the inner corner of the eyelid.
Frequently misdiagnosed. Because it mimics a persistent one-sided conjunctivitis, canaliculitis is often missed for months. See the dedicated Canaliculitis page for clinical photos, diagnosis, and the curative canaliculotomy with curettage.
Inflammation or infection of the lacrimal gland presents with tenderness and swelling of the outer upper eyelid. Viral causes include mumps, Epstein-Barr virus, and herpes zoster. Systemic conditions such as sarcoidosis, Sjögren’s syndrome, and lymphoma can produce a similar picture and must be excluded during evaluation.
Molluscum contagiosum is a common viral skin infection caused by the molluscum contagiosum virus (MCV), a DNA poxvirus. On the face and eyelids it produces characteristic small, flesh-colored, dome-shaped papules with a central dimple (umbilication).



When molluscum lesions involve the eyelid margin, viral particles shed into the tear film and trigger a chronic follicular conjunctivitis. The conjunctivitis will not resolve until the eyelid lesions are treated.


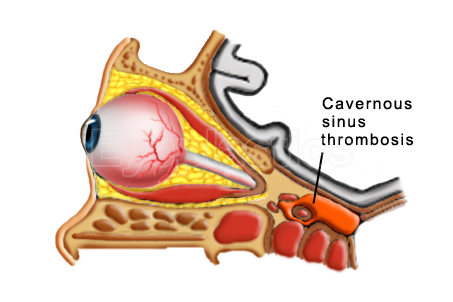
The Chandler classification provides a clinically useful staging system for periorbital and orbital infections:
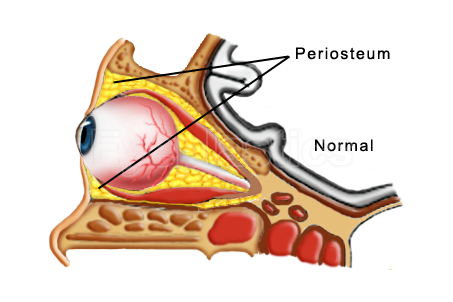
Step 1 of 5
Normal orbit — the orbital septum and periosteum keep the eye, fat and muscles compartmentalized.
Drag the slider to follow how an untreated orbital infection can progress through the Chandler stages.
Rhino-orbital-cerebral mucormycosis is a rare but rapidly fatal opportunistic fungal infection caused by fungi of the order Mucorales. It almost exclusively affects patients with poorly controlled diabetic ketoacidosis or severe immunocompromise.
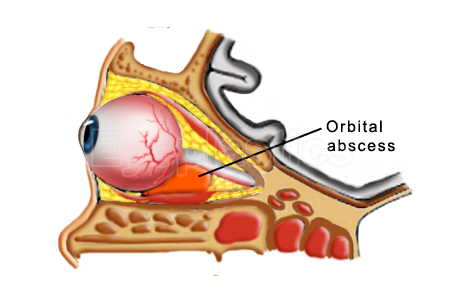
An orbital abscess is a collection of pus within the orbital fat, typically arising from untreated or inadequately treated orbital cellulitis (Chandler stage IV). It demands urgent surgical drainage to prevent permanent vision loss.
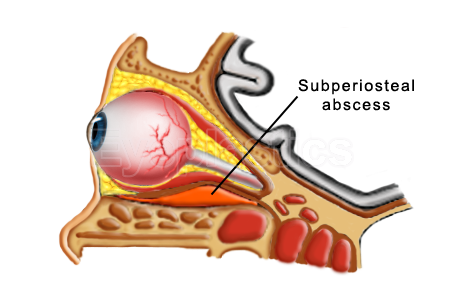
A subperiosteal abscess (SPA) forms between the bony orbital wall and the periorbita, most commonly on the medial wall from ethmoidal sinusitis. It is the most common orbital complication of sinusitis in children.
Schedule a consultation with Andrew M. Goldbaum, MD to learn if this procedure is right for you.