Eyelid
Blepharoplasty
Upper and lower eyelid blepharoplasty ("eye lift") — cosmetic and functional correction of excess eyelid skin and fat.
Medically reviewed by Andrew M. Goldbaum, MDOculoplastic SurgeonLast updated June 2026
Eyelid
Upper and lower eyelid blepharoplasty ("eye lift") — cosmetic and functional correction of excess eyelid skin and fat.
Medically reviewed by Andrew M. Goldbaum, MDOculoplastic SurgeonLast updated June 2026
Blepharoplasty is surgery to reshape the upper eyelid, lower eyelid, or both by removing or repositioning excess skin, muscle, and fat. It may be performed for functional reasons — when excess upper lid skin obstructs the superior visual field — or for cosmetic improvement of a tired or aged appearance. Most blepharoplasties are done under local anesthesia with sedation as outpatient procedures.
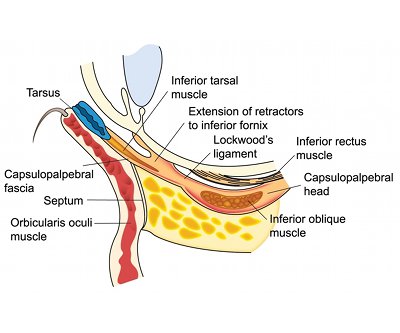
For a detailed guide to eyelid anatomy, see our dedicated Eyelid Anatomy page.
Good candidates for eyelid surgery are adults in reasonable general health who are bothered by excess upper-lid skin, puffy lower-lid bags, or a heavy, tired appearance that no longer matches how they feel. Blepharoplasty corrects skin, muscle, and fat — it does not lift the eyebrow, erase fine crow’s-feet, or treat a drooping lid margin caused by a weak levator muscle. Understanding which structure is actually responsible for the tired look is the single most important step before surgery, because the wrong operation will not fix the problem.
Upper-eyelid surgery falls into two categories that often overlap:
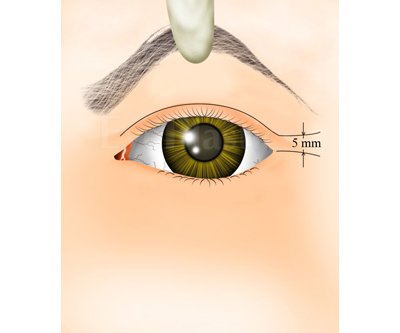
A droopy upper lid is not always a skin problem. If the eyelid margin itself sits low — when the distance from the pupil light-reflex to the upper-lid margin (MRD-1) is about 4–5 mm normally and drops to 2 mm or less — the cause is ptosis, a stretched or weak levator muscle, and it needs a different repair. Many patients have both excess skin and true ptosis and benefit from combining the two operations. See Ptosis vs. Blepharoplasty for how surgeons tell them apart.
Eyelid surgery is tailored to which lids are involved and what needs correcting. Explore each procedure in depth:
Choose a section, then drag the slider to step through it.
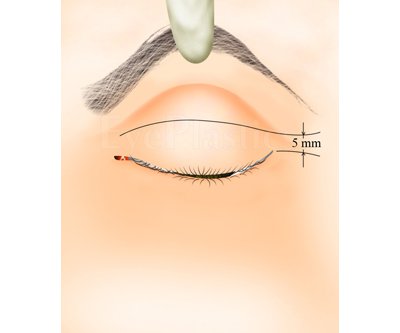
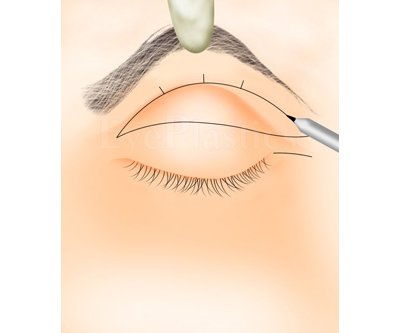
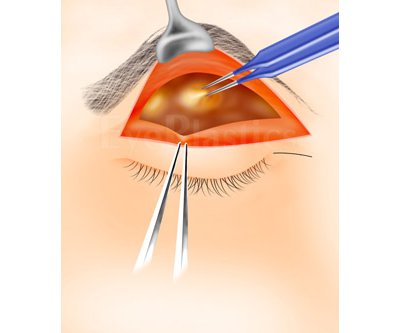
Step 1 of 9
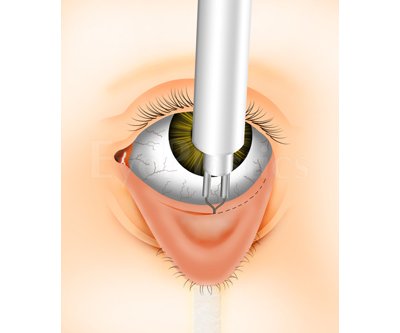
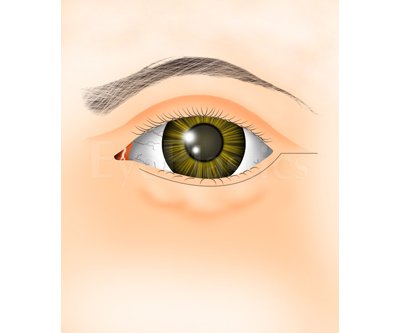
Skin incision is marked within the crease of the eyelid
Drag the slider to compare
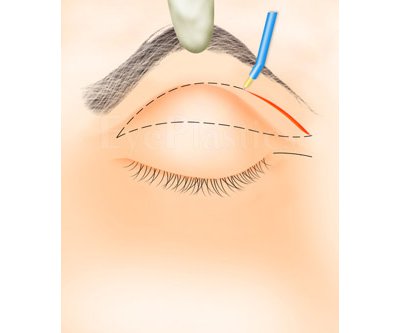
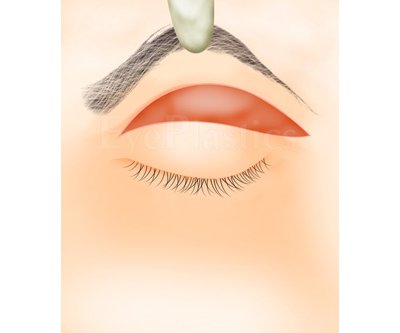
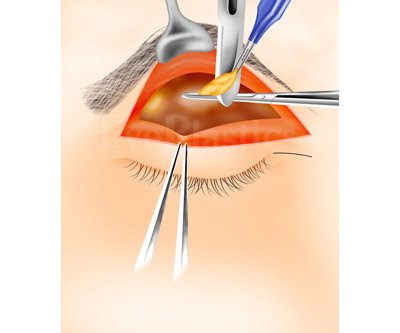
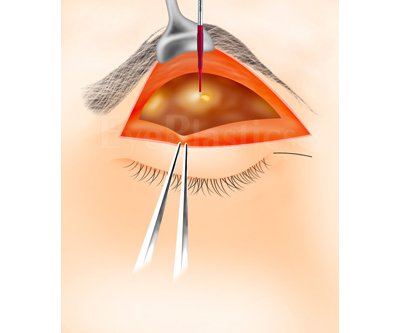
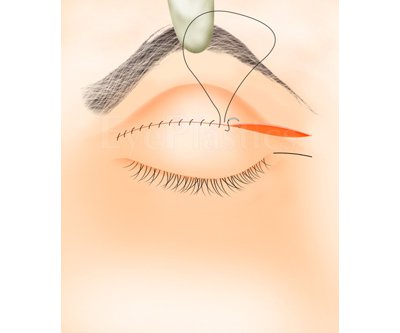
Blepharoplasty is performed through external incisions placed along the natural skin lines of the eyelids — the crease of the upper lid, or below the lashes of the lower lid — or through the inner conjunctival surface (transconjunctival blepharoplasty). The surgeon removes excess skin, trims or repositions fat, and tightens supporting structures before closing incisions with fine sutures.
The operation typically takes one to three hours depending on the number of lids treated and the techniques used. After surgery, swelling and bruising are expected for 7–14 days; the final result is typically stable by 3 months.
Swelling and bruising peak at 48 hours and resolve substantially over 1–3 weeks. The progression below shows a typical upper blepharoplasty recovery.



Patients of Asian heritage may benefit from a specialized technique — see Asian Blepharoplasty for details on double-eyelid surgery and pretarsal crease creation.
The upper face ages as a unit, so blepharoplasty is frequently discussed alongside — and sometimes combined with — neighboring procedures. Choosing correctly depends on what is actually descending:
Cosmetic blepharoplasty is an out-of-pocket expense, and the total varies with geography, the surgeon’s experience, whether one or both lids are treated, and facility and anesthesia fees. Functional upper-lid surgery may be covered when a visual-field test confirms that hooding skin obstructs the superior field; Dr. Goldbaum’s office documents this and seeks pre-authorization. One important nuance: when blepharoplasty is performed at the same session as ptosis repair, the skin (blepharoplasty) portion is considered cosmetic even if the ptosis repair is covered. Ask for an itemized estimate that separates surgeon, facility, and anesthesia fees. For typical prices, the medical-necessity criteria in detail, and payment options, see our Eyelid Surgery Cost & Insurance guide and Is Blepharoplasty Covered by Insurance?
Most blepharoplasties are outpatient procedures done under local anesthesia with light intravenous sedation — you are relaxed and comfortable but not under general anesthesia, which shortens recovery and lowers risk. You arrive having avoided blood thinners and aspirin-type medications for the interval Dr. Goldbaum specifies, the lids are marked while you sit upright, and you go home the same day with someone to drive you. Plan to keep your head elevated and apply cold compresses that first evening.
The eyelids are delicate, functionally critical structures millimeters from the eye itself, and the difference between an excellent and a disappointing result is often surgical judgment about how little to remove. Blepharoplasty is most safely performed by an oculoplastic surgeon — a physician with combined training in ophthalmology and plastic surgery of the eyelids and orbit. Surgeons who are ASOPRS fellowship-trained (American Society of Ophthalmic Plastic and Reconstructive Surgery) manage eyelid anatomy, tear function, and complications every day. Ask about board certification, how many blepharoplasties the surgeon performs annually, and review before-and-after photographs of their own patients. You can find fellowship-trained surgeons through our surgeon directory.
Upper-eyelid blepharoplasty is durable: results are typically stable at three months and often last 10+ years, though the lids continue to age slowly like the rest of the face. Lower-eyelid results are more variable. Blepharoplasty does not stop aging, but for most patients a single well-planned operation delivers a long-lasting, natural refresh rather than a “done” look.
Blepharoplasty is a commonly performed and generally well-tolerated facial procedure, but every operation carries risk. Being well informed before surgery — and choosing an ASOPRS-trained oculoplastic surgeon who manages these structures daily — is the best protection. The complications below range from common and self-limited to rare but serious.
1Pain, swelling & bruising
Expected after any eyelid surgery and almost always temporary. Cold compresses, head elevation, avoiding anticoagulants beforehand, and blood-pressure control minimize ecchymosis and hematoma.
2Scarring
Incisions are hidden in the lid crease and typically fade to a faint line. Keloid-prone patients may develop thickened or pigment-changed scars.
3Wound dehiscence
A wound that re-opens — usually from rubbing, restless sleep, or minor trauma. Careful suture technique and post-operative precautions prevent most cases.
4Upper-lid overcorrection / lagophthalmos
Removing too much skin can leave the eye unable to close fully, causing exposure and dryness. Conservative skin excision is the rule, especially after prior trauma or in thyroid eye disease.
5Lower-lid retraction & ectropion
The most visible lower-lid complication: the lid is pulled down or turns outward from skin shortage or scarring (photos below). Often requires lid-tightening or graft revision.
6Asymmetry
Small differences in crease height or fold are the most common reason for touch-up surgery; meticulous preoperative marking minimizes the risk.
7Dry-eye syndrome
Pre-existing dry eye can worsen after eyelid surgery; tear function should be assessed beforehand and treated aggressively afterward.
8Diplopia (double vision)
Very rare — from injury to an extraocular muscle (most often the inferior oblique) during lower-lid fat removal. Usually transient; persistent cases are treatable.
9Ocular injury
The eye itself is immediately adjacent to the surgical field; corneal abrasion or (extremely rarely) deeper injury can occur.
10Retrobulbar hemorrhage & vision loss
The most feared complication: bleeding behind the eye that can compress the optic nerve. Hemorrhage is rare (on the order of 1 in 2,000) and permanent vision loss is rarer still (roughly 1 in 20,000). It is treated as an emergency — the reason eyelid surgery belongs in experienced hands.



Perspective: serious complications are rare, and most of those shown above are correctable with revision surgery. Discuss your individual risk profile — medications, dry eye, thyroid disease, prior surgery — with Dr. Goldbaum before the procedure.
Although both are called "eyelid surgery," upper and lower blepharoplasty solve different problems with different techniques, incisions, and recovery. Matching the operation to the anatomy is what separates a natural result from an operated look.
| Upper blepharoplasty | Lower blepharoplasty | |
|---|---|---|
| Primary concern | Hooding/redundant skin over the crease; heaviness | Under-eye bags, fat prolapse, crepey skin |
| Incision | Hidden in the natural lid crease | Below the lashes, or hidden inside the lid (transconjunctival) |
| Fat handling | Conservative removal; skin is the main target | Repositioned or selectively removed to smooth the lid-cheek junction |
| Insurance | May be covered when a visual-field test documents obstruction | Almost always cosmetic (out of pocket) |
| Durability | Long-lasting — often 10+ years | More variable; volume and skin quality keep evolving |
The two are frequently combined in a single session (four-lid blepharoplasty). The decision is anatomic, not menu-driven: a heavy upper lid caused by a dropped brow needs a brow lift, not more skin removal, and a low lid margin needs ptosis repair rather than a skin operation.
In eyelid surgery the most common regret is not "too little done" but "too much taken." A trained oculoplastic surgeon plans around three principles: preserve enough skin for the eye to close fully (avoiding lagophthalmos and exposure), keep or reposition fat rather than hollowing the socket, and respect the fellow eye so the two match. Because the tissues heal and settle over three months, conservative surgery with a planned minor touch-up beats aggressive surgery that cannot be undone. This surgical judgment — not a single technique — is why eyelid surgery belongs with an ASOPRS-trained specialist who operates on these structures daily.
This page is the hub of an in-depth library on eyelid surgery. Explore each part:
Schedule a consultation with Andrew M. Goldbaum, MD to learn if this procedure is right for you.